|
|
|
|
|
Symptomatic Transverse Colon Lipoma
|
|
|
|
Vijay Kumar Sharma, Ashok Kumar, Anu Behari, Alister J Victor Department of Surgical Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Science, Lucknow-226014, Uttar Pradesh, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr. Ashok Kumar Email: drashok97@gmail.com |
|
|
|
|
|
|
|
|
Received:
06-JUL-2022 |
Accepted:
22-APR-2023 |
Published Online:
15-MAY-2023 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Background: Colonic lipomas are rare benign neoplasms within the gastrointestinal tract. They are often asymptomatic but can cause abdominal pain and other symptoms when they exceed 2 cm. Diagnosis involves imaging and colonoscopy, while surgical excision is recommended for symptomatic cases. Case Report: A 48-year-old female patient with a medical history of hypothyroidism and hypertension presented with colicky abdominal pain, nausea, and vomiting. Imaging revealed a large lipoma in the transverse colon, confirmed by colonoscopy. Surgical excision was performed, resulting in symptom resolution. Conclusion: Awareness of colonic lipomas and their potential for symptomatic presentation and role of imaging techniques is important for prompt diagnosis and appropriate management. |
|
|
|
|
|
Keywords :
|
Abdominal Pain, Colonic Lipoma, Imaging Techniques, Transverse Colon, Vomiting.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ffec173a0000005f07000001000600 Introduction
Gastrointestinal tract lipomas are uncommon benign neoplasms that do not originate from epithelial cells. Among gastrointestinal lipomas, colonic lipomas are the most prevalent, accounting for approximately 65-75% of cases [ 1]. The first documented case of a colonic lipoma was reported by Bauer in 1757 [ 1]. The incidence of colonic lipomas ranges from 0.2% to 4.4% [ 2]. The majority of colonic lipomas are asymptomatic and usually measure less than 2 cm in size [ 3]. While lipomas themselves do not undergo malignant transformation, some cases may exhibit atypical pseudosarcomatous features on histology [ 4]. When colonic lipomas exceed 2 cm, common presentations include abdominal pain, altered bowel habits, and gastrointestinal bleeding [ 5]. Among the colonic segments, the ascending colon (45%) is the most frequently affected site, followed by the sigmoid colon (30%), descending colon (15%), and transverse colon (9%) [ 6]. The detection of colonic lipomas can be achieved using endoscopic or radiologic techniques such as computed tomography (CT) or magnetic resonance imaging (MRI). Histologically, these lesions typically display well-circumscribed mature adipose tissue with normal mucosal covering or may contain an adenoma or a serrated polyp [7]. Surgical excision is typically recommended to alleviate symptoms and exclude the possibility of malignancy. In this case report, we present the clinical manifestation, diagnostic evaluation, and surgical management of a symptomatic transverse colon lipoma in a 48-year-old female patient.
Case Report
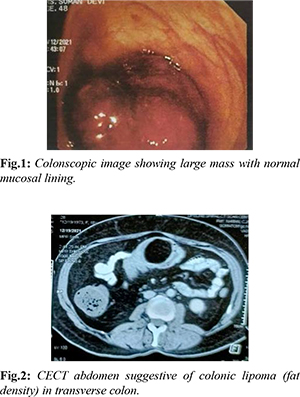
A 48-year-old female patient, who had a known medical history of hypothyroidism and hypertension, presented to our medical facility with colicky abdominal pain in the umbilical and left lower abdomen. The pain was of moderate to severe intensity and accompanied by nausea and vomiting. The pain exacerbated after meals and was alleviated with analgesics. The patient reported having made dietary modifications and using laxatives for the past two months. Notably, there was no history of diarrhea, hematochezia, or melena. Abdominal examination did not reveal any significant findings. Routine laboratory tests, including complete blood count, renal function test, liver function test, and serum carcinoembryonic antigen levels, were all within normal limits. In order to further investigate the patient's condition, an ultrasound of the abdomen, followed by a computed tomography (CT) scan of the abdomen and a subsequent colonoscopy, were performed. The CT scan indicated thickening and distension of the transverse colon, along with the presence of a large, globular fatty lesion measuring approximately 6×5 cm. Additionally, thickening of the gallbladder wall was observed [Fig.1]. During the colonoscopy, a large mass lesion obstructing the lumen of the transverse colon was visualized. The lesion exhibited a smooth surface, and the scope was unable to pass through it proximally [Fig.2]. A biopsy of the colon, obtained during the colonoscopy, revealed no evidence of dysplasia or malignancy.
Due to the persistence of symptoms and the presence of a sizable mass on the imaging studies, the patient underwent surgery. Intraoperatively, a palpable mass was identified in the transverse colon. Consequently, the patient underwent segmental colectomy, primary colo-colic anastomosis, and cholecystectomy. Upon gross examination, the resected mass appeared as a large pedunculated lesion measuring 7×5 cm, with a normal mucosal surface and ulceration. On cut section, the mass appeared soft and homogeneously yellow in color [Fig.3]. Histopathological examination confirmed the diagnosis of colonic lipoma and chronic cholecystitis [Fig.4]. The patient experienced an uneventful post-operative course and was discharged on the sixth day following surgery.
Discussion
Colonic lipomas are often asymptomatic and incidentally discovered during routine diagnostic procedures. Most lipomas are small, measuring less than 2 cm in size, and rarely cause symptoms [ 3]. However, when they exceed 2 cm, they can present with abdominal pain, altered bowel habits, or gastrointestinal bleeding [ 5]. In our case, the patient experienced colicky abdominal pain in the umbilical and left lower abdomen, which prompted further investigation. Imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) play a crucial role in the diagnosis of colonic lipomas. CT scans can reveal characteristic findings such as thickening and distension of the affected colon segment, along with the presence of a large globular fatty lesion [7]. In our case, the CT scan demonstrated thickening and distension of the transverse colon, with a large globular fatty lesion measuring approximately 6×5 cm. These findings were consistent with a colonic lipoma. Colonoscopy is another valuable tool for diagnosing colonic lipomas, allowing direct visualization of the lesion and obtaining biopsy samples if needed. During colonoscopy, a large mass obstructing the lumen of the transverse colon was identified in our patient. Biopsy results showed no evidence of dysplasia or malignancy, supporting the diagnosis of a benign colonic lipoma. Histopathological examination of the resected specimen confirmed the diagnosis of colonic lipoma. The gross examination revealed a large pedunculated mass covered with normal mucosal surface ulceration. Microscopically, colonic lipomas display well-circumscribed mature adipose tissue with overlying normal mucosa [7]. In our case, the histopathological analysis was consistent with colonic lipoma. Surgical excision is usually recommended for symptomatic colonic lipomas to relieve symptoms and exclude the possibility of malignancy. In our case, the patient underwent segmental colectomy and cholecystectomy, which resulted in a successful resolution of symptoms. The post-operative course was uneventful, and the patient was discharged on the sixth day after surgery.
Conclusion
This case report highlights the clinical presentation, diagnostic evaluation, and surgical management of a symptomatic transverse colon lipoma. The use of imaging modalities such as CT and colonoscopy proved invaluable in establishing the diagnosis. Surgical intervention was effective in alleviating the patient's symptoms and confirming the benign nature of the lesion. Awareness of colonic lipomas and their potential for symptomatic presentation is important for prompt diagnosis and appropriate management.
Contributors: VKS: Preparation of manuscript, literature search; AK: analysis, design, interpretation; AB: critical review of manuscript; AJV: literature search. AK will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study. Funding: None; Competing interests: None stated.
References - Zhang H, Cong JC, Chen CS, Qiao L, Liu EQ. Submucous colon lipoma: a case report and review of the literature. World J Gastroenterol. 2005;11:3167-3169.
- Zeebregts CJ, Geraedts AA, Blaauwgeers JL, Hoitsma HF. Intussusception of the sigmoid colon because of an intramuscular lipoma. Report of a case. Dis Colon Rectum. 1995;38:891-892.
- Presti ME, Flynn MF, Schuval DM, Vollmar TM, Zotos VD. Colonic lipoma with gastrointestinal bleeding and intussusception. ACG Case Rep J. 2015;2:135-136.
- Sapalidis K, Laskou S, Kosmidis C, Passos I, Mantalobas S, Michalopoulos N, et al. Symptomatic colonic lipomas: Report of two cases and a review of the literature. SAGE Open Med Case Rep. 2019;7:2050313X19830477.
- Mason R, Bristol JB, Petersen V, Lyburn ID. Lipoma induced intussusception of the transverse colon. J Gastroenterol Hepatol. 2010;25:1177.
- Jiang L, Jiang LS, Li FY, Ye H, Li N, Cheng NS, Zhou Y. Giant submucosal lipoma located in the descending colon: a case report and review of the literature. World J Gastroenterol. 2007;13:5664-5667.
- Bardají M, Roset F, Camps R, Sant F, Fernández-Layos MJ. Symptomatic colonic lipoma: differential diagnosis of large bowel tumors. Int J Colorectal Dis. 1998;13:1-2.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Sharma VK, Kumar A, Behari A, Victor AJSymptomatic Transverse Colon Lipoma.JCR 2023;13:46-48 |
|
Sharma VK, Kumar A, Behari A, Victor AJSymptomatic Transverse Colon Lipoma.JCR [serial online] 2023[cited 2024 Dec 21];13:46-48. Available from: http://www.casereports.in/articles/13/2/Symptomatic-Transverse-Colon-Lipomaa.html |

|
|
|
|
|