Introduction
Lumbar hernias are protrusion of abdominal viscus or part of viscus through a defect in lumbar triangle. Congenital lumbar hernia is a rare entity of which one third are isolated and two third are associated with other congenital anomalies including vertebrae, ribs, caudal regression syndrome, ureter pelvic junction obstruction, renal agenesis where lumbocostovertebral syndrome are the most common [1]. It may be asymptomatic at birth or presents as a visible swelling more pronounced on crying. Here we are reporting a case of congenital lumbar hernia with lumbocostovertebral syndrome which is a rare entity with only 60 cases reported so far [2].
Case Report
A one and a half-month-old baby boy presented to the Pediatric Surgery OPD with a mass in the right flank region, present since birth [Fig.1]. The mass had been gradually increasing in size and became more pronounced when the baby cried. The baby was born at 39 weeks to a 22-year-old mother following an uncomplicated pregnancy and a normal vaginal delivery. No resuscitation was required at birth. He is the second child of non-consanguineous parents, with an elder brother who is currently 3 years old and has met all developmental milestones.

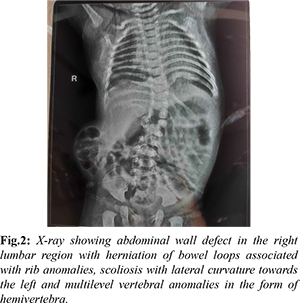
On physical examination, there was a visible swelling in the right lumbar region, approximately 8×6 cm in size, soft in consistency with intact overlying skin, and reducible. The swelling appeared more prominent when the baby cried. The rest of the systemic examination was within normal limits. Chest and abdominal X-rays revealed an abdominal wall defect in the right lumbar region with herniation of bowel loops, rib anomalies, scoliosis, and hemivertebra [Fig.2]. An ultrasound of the abdomen and pelvis revealed a focal defect of approximately 25 mm in the right lumbar region through which bowel loops were herniating. Other solid organs were normal.
For surgery, the patient was positioned in the left lateral position. An incision was made transversely over the hernia site in the right lumbar region. The hernial sac contained bowel loops, which were reduced [Fig.3]. After defining the edges of the defect, the final size was measured to be approximately 3×2 cm. A space was created between the peritoneum and the muscle layer, and a 5×4 cm polypropylene mesh was placed [Fig.4]. The muscle layer was then sutured in two layers, followed by the subcutaneous tissue and skin. The post-operative period was uneventful, and the patient was discharged on post-operative day 4.
Discussion
Lumbar hernias, first reported by Dr. Garangeot in 1731 and further elaborated by Petit in 1783 and Grynfeltt in 1866, are rare anatomical defects characterized by the protrusion of abdominal contents through the lumbar triangle [3]. These hernias are classified based on their anatomical location: the superior lumbar triangle of Grynfeltt or the inferior lumbar triangle of Petit. The superior triangle is bounded laterally by the posterior border of the internal oblique muscle, medially by the quadratus lumborum and erector spinae muscles, and superiorly by the 12th rib. The inferior triangle is bordered anteriorly by the external oblique muscle, posteriorly by the latissimus dorsi, and inferiorly by the iliac crest [4].
Etiologically, lumbar hernias can be congenital or acquired. Congenital lumbar hernias, comprising about 20% of cases, result from developmental defects in the musculoskeletal system, potentially due to transient anoxia during gestational weeks 3-5 or congenital weak points in the superior lumbar triangle. Acquired hernias, which make up 80% of cases, often arise secondary to trauma, surgery, or inflammation [5,6].
Diagnostically, a computed tomography (CT) scan of the abdomen and pelvis is the gold standard for identifying lumbar hernias, offering detailed imaging of the herniated contents and associated structural anomalies [7]. In our case, imaging revealed a right lumbar region defect with herniation of bowel loops, rib anomalies, scoliosis, and hemivertebrae, consistent with lumbocostovertebral syndrome.
Surgical intervention is crucial for lumbar hernias due to the high risk of complications such as incarceration (25%) and strangulation (10%). The primary goals of surgery are to reduce the hernial sac, repair the defect, and reinforce the posterior abdominal wall. Techniques vary from simple anatomical closure to more complex repairs using musculofascial flaps or prosthetic mesh. Evidence suggests that the use of extraperitoneal prosthetic mesh is particularly effective, as it avoids the need for bony anchorage and reduces the risk of injury to underlying structures. While laparoscopic approaches offer technical advantages, the open method remains the preferred technique due to its established efficacy [8-11].
Conclusion
Congenital lumbar hernia with lumbocostovertebral syndrome is a rare but significant condition in pediatric patients. Prompt diagnosis and surgical intervention are essential to prevent complications and address associated anomalies. Open prosthetic repair remains the gold standard, offering a reliable and effective solution for these complex hernias. Surgeons should be vigilant for other congenital anomalies in patients presenting with congenital lumbar hernia, ensuring comprehensive management and optimal outcomes.
Contributors: NMT: Case details, contributed to the design of the report and drafted the manuscript. DDS: Case details and report designing; MS, AT: critical inputs into the manuscript. NMT will act as a study guarantor. All authors approved the final version of this manuscript and are responsible for all aspects of this study.
Funding: None; Competing interests: None stated.
References
- Sengar M, Manchanda V, Mohta A, Jain V, Das S. Intercostal variant of lumbar hernia in lumbocostovertebral syndrome: our experience with 6 cases. J Pediatr Surg. 2011;46(10):1974-1977.
- Akçora B, Temiz A, Babayigit C. A different type of congenital lumbar hernia associated with the lumbocostovertebral syndrome. J Pediatr Surg. 2008;43(1):e21-23.
- De Garangeot RJC. Traite des operations de chirurgie. Teratology. 1731;1:369.
- Guillem P, Czarnecki E, Duval G, Bounoua F, Fontaine C. Lumbar hernia: anatomical route assessed by computed tomography. Surg Radiol Anat. 2002;24(1):53-56.
- Touloukian RJ. The lymbocostovertebral syndrome: a single somatic defect. Surgery. 1972;71(2):174-181.
- Lesshaft P. Die Lumbalgegend in anatomisch-chirurgischer Hinsicht. Archiv für Anatomie, Physiologie und wissenschaftliche Medicin. 1870;264-299.
- Moreno-Egea A, Baena EG, Calle MC, Maritnez JAT, Albasani JSA. Controversies in the current management of lumbar hernias. Arch Surg. 2007;142:82-88.
- Moreno-Egea A, Alcaraz AC, Cuervo MC. Surgical options in lumbar hernia: laparoscopic versus open repair. A long-term prospective study. Surg Innov. 2013; 20:331-344.
- Lim MS, Lee HW, Yu CH, Yang DH. Laparoscopic total extraperitoneal repair of lumbar hernia. J Korean Surg Soc. 2011;81:287-290.
- Yavuz N, Ersoy YE, Demirkesen O, Tortum OB, Erguney S. Laparoscopic incisional lumbar hernia repair. Hernia. 2009;13:281-286.
- Suarez S, Hernandez JD. Laparoscopic repair of a lumbar hernia: report of a case and extensive review of the literature. Surg Endosc. 2013;27:3421-3429.