|
|
|
|
|
Renal Cell Carcinoma with Osseous Metaplasia
|
|
|
|
Divya Kriplani, Priti P Trivedi, Manoj J Shah
From the Department of Pathology, The Gujarat Cancer and Research Institute,
Ahmedabad - 380016, Gujarat, India. |
|
|
|
|
|
Corresponding Author:
|
|
Dr. Divya Kriplani
Email: divya_krips@yahoo.co.in |
|
|
|
|
|
|
|
|
Received:
2-MAY-2013 |
Accepted:
24-MAY-2013 |
Published Online:
10-JUN-2013 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Focal calcifications are not an uncommon occurrence in renal masses. Osseous metaplasia however, is a rare finding. We report a case of large renal mass with radiological evidence of calcification. Histopathological examination showed clear cell renal cell carcinoma with osseous metaplasia. |
|
|
|
|
|
Keywords :
|
Renal Cell Carcinoma, Calcinosis, Kidney, Kidney Neoplasms, Calcification, Metaplasia.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff942103000000cf01000001000900 6go6ckt5b5idvals|203 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Renal cell carcinoma accounts for 2% of total human cancers [ 1], and the clear cell variant represents the most common histological subtype. Albrecht reported the first case of calcified renal cell carcinoma in 1905 [ 2]. All variants of renal cell carcinoma (RCC) may exhibit necrosis and hemorrhage. Other degenerative changes that can be seen are edema, fibrosis, cholesterol clefts and calcification. Computerized Tomography (CT) demonstrates calcification in 31% of RCCs [ 3]. Osseous metaplasia in RCC is, however a rare phenomena. We report the case of a clear cell variant of RCC showing osseous metaplasia.
Case Report
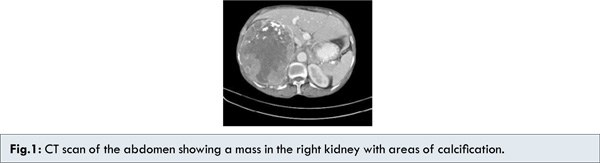
A 55 year old female presented with complaint of pain in right loin for last one month. She had no urinary complaints. She had no other significant past or family history. Her abdomen examination revealed a mass in the right hypochondrium which was firm, nontender, bimanually palpable and moved with respiration. An ultrasound abdomen showed a soft tissue mass lesion in the right lumbar region displacing the kidney anteroinferiorly. A CT scan abdomen and pelvis showed a 14×12 cm lobulated, heterogeneously enhancing soft tissue density lesion involving almost entire right kidney and sparing a small part of the lower pole. Lesion showed internal necrosis with multiple specks of calcification and capsular calcification [Fig. 1]. Lesion involved the right renal hilum with compression of the renal vein. Multiple enlarged nodes were noted in the pre-aortic, para-aortic and lower aorto-caval region. The left kidney, liver, spleen and pancreas were normal. The uterus and bilateral adnexa were also normal. A Doppler study was done which showed a large mass arising from the kidney. The lesion encased the right renal vein and was compressing and displacing the inferior vena cava (IVC). Thrombosis was noted in the right renal vein extending up to the junction of renal vein and IVC, but further extension into IVC was not seen. A chest X-ray showed soft tissue opacity in the right middle zone. A CT thorax was done which showed few nodular soft tissue opacities in the left lower lobe and right middle lobe, largest measuring 1×1 cm. These were suggestive of pulmonary metastases. Few enlarged axillary lymph nodes were noted bilaterally. Trachea and main bronchi were normal. There was no other lymphadenopathy and no pleural effusion. The patient underwent a right radical nephrectomy.
Grossly, the kidney was externally well encapsulated. On cutting almost entire kidney was replaced by a growth having a friable tan cut surface with intervening hard areas. Extensive areas of hemorrhage and necrosis were seen. Cut end renal vessels and ureter were free of tumor. On microscopic examination, the tumor showed cells arranged in nests and tubules having irregular nuclei, prominent nucleoli and abundant pale to eosinophilic cytoplasm. Multinucleated tumor giant cells were seen. It was associated with extensive areas of hemorrhage, necrosis and area of osseous metaplasia [Fig.2,3]. Capsule was intact and perinephric fat was free of tumor. No embolus was seen in the renal vessels and hilar lymph nodes were not found. Based on the overall morphologic features the final diagnosis of clear cell RCC (Fuhrman grade IV) with osseous metaplasia was made.
Discussion
Calcification can be seen in both benign and malignant renal lesions. Differential diagnosis for calcified renal mass includes RCC, Wilms tumor, oncocytoma, metanephric adenoma [ 4], angiomyolipoma, intra renal aneurysms, cystic renal disease, renal abscess, echinococcal cysts, schistosomiasis, tuberculosis, xanthogranulomatous pyelonephritis, arteriovenous malformations and hematoma [ 5]. Osseous metaplasia opposed to calcification is a rare finding. It has been demonstrated in several other tumors, including primary and metastatic colorectal carcinomas predominantly in mucinous tumors, benign rectal polyps, endometrioid carcinoma of the fallopian tube, malignant melanoma, breast carcinoma, hepatocellular carcinoma, amyloid tumors of the breast and tonsil, fibrous histiocytoma and perineuroma [ 6].
The pathogenesis of ossification in tumors is not clear. Several hypotheses have been put forward, including the production of bone by tumor cells secondary to ischemia, necrosis or inflammation in the tumor or surrounding tissue, reparative responses in the tumor or surrounding tissues or the ossification of pre existing mucin or calcification foci. A recent study has shown, Bone morphogenetic protein 2 (BMP2) to inhibit tumor growth of RCC and induce bone formation [ 7].
The prognostic significance of osseous metaplasia in RCC is debatable. Some reports show ossification to be a favorable prognostic factor with tumors having a low nuclear grade, low stage and absence of metastatic disease at presentation [ 4, 6, 8]. However, some reports suggest that ossification can also be associated with high grade tumors and poor prognosis [ 9], similar to our patient, who had a high nuclear grade, high stage and presence of pulmonary metastases at the time of presentation. The patient’s long-term outcome remains to be determined.
In summary, we report a case of clear cell renal cell carcinoma (Fuhrman grade IV) with osseous metaplasia and pulmonary metastases at presentation. While osseous metaplasia is a rare event in renal cell carcinomas, it has been reported in tumors with both low grade and high-grade nuclear features. This indicates that contrary to some reports suggesting a better prognosis for these tumors, it may not have any significant prognostic impact and is only an unusual associated finding.
References
- Eble JN, Sauter G, Epstein JI, Sesterhenn IA (Eds): WHO classification of tumors. Pathology and genetics of tumors of the urinary system and male genital organs. IARC press: Lyon 2004.
- Albresht P. Und pathologischen anatomie der malignen hypernephrome. Arch F Klin Chir. 1905;77:1072.
- Murugan P, Basu D, Manikandan R, Dorairajan LN, Kumar S. osseous mtaplasia in renal cell carcinoma: Report of a rare case. Ind J Pathol Micro. 2008;51:399-401.
- Hartman Jr RJ, Helfand BT, Dalton DP. Clear cell renal cell carcinoma with osseous metaplasia: a case report. Can J Uro. 2011;18:5564-5567.
- Ozkanli S, Yildirim A, Zemheri E, Kaskin SK, Basok EK. Osseous metaplasia and bone marrow elements in a case of renal cell carcinoma. Case Rep Urol. 2012;2012:649257.
- Cribbs RK, Ishaq M, Arnold M, O’Brien J, Lamb J, Frankel WL. Renal Cell Carcinoma with massive osseous metaplasia and bone marrow elements. Ann Diagn Pathol. 1999;3:294-299.
- Wang L, Park P, Zhang H, La Marca F. Bone morphogenetic protein 2 inhibits tumor growth of human renal cell carcinomas and induces bone formation. Int J Cancer. 2012;131:1941-1950.
- Singh V, Sinha RJ, Sankhwar SN, Dalela D. Heterotopic bone formation in renal cell carcinoma: A diagnostic challenge. Ind J Cancer. 2008;45:126-127.
- O. Bielsa, J. Loreta, O. Arango, S. Serrano, A. Gilbert-Mas. Bone metaplasia in a case of bilateral renal cell carcinoma. Urol Int. 2001;66:55–56.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Kriplani D, Trivedi PP, Shah MJRenal Cell Carcinoma with Osseous Metaplasia.JCR 2013;3:165-168 |
|
Kriplani D, Trivedi PP, Shah MJRenal Cell Carcinoma with Osseous Metaplasia.JCR [serial online] 2013[cited 2026 Jun 20];3:165-168. Available from: https://www.casereports.in/articles/3/1/renal-cell-carcinoma.html |

|
|
|
|
|