|
|
|
|
|
Unruptured Intracranial Aneurysm Involving the Distal Anterior Cerebral Artery: A Cadaveric Study
|
|
|
paroxetine 20 paroxetine effet S. Allwyn Joshua, Sheela G Nayak, V S Pare, Ashok1, Roopa Sebastian1
From the Department of Anatomy and Biochemistry1, K V G Medical college,
Sullia, Karnataka, India |
|
|
|
|
|
Corresponding Author:
|
Dr. S. Allwyn Joshua
Email: oxfordjosh@yahoo.com |
|
|
|
|
|
|
|
|
Received:
21-NOV-2012 |
Accepted:
23-DEC-2012 |
Published Online:
05-JAN-2013 |
|
|
|
|
|
|
|
Abstract
|
|
|
|
Aneurysm affecting the distal segment of anterior cerebral artery (DACA) are well documented. But scanty literature is available on the structural and morphological changes produced by the aneurysm on the brain tissue which in turn can produce clinical effects and functional disturbances. Distal cerebral artery aneurysms represent 1.5% to 9% of intracranial aneurysms and most often occur at the origin of the calloso-marginal artery. Frontal lobe plays a vital role in higher mental functions such as motivation, planning, social behaviour and speech production. Damage to frontal lobe can show cognitive, emotional, behavioural symptoms. We present a case report of a completely thrombosed unruptured intracranial aneurysm (UIAs) of anterior cerebral artery proximal to origin of calloso-marginal artery in a cadaveric brain. This space occupying lesion in this particular case may be considered as one of cause for progressive frontal lobe syndrome. Therefore, it is desirable to identify UIA’s which are at greater risk of rupture and those which may cause slow progressive space occupying lesion, while considering which to repair. |
|
|
|
|
|
Keywords :
|
Intracranial Aneurysm, Frontal Lobe, Anterior Cerebral Artery, Speech, Behavioral Disorders.
|
|
|
|
|
|
|
|
|
|
|
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1fff417020000000f01000001001700 6go6ckt5b5idvals|164 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Anterior cerebral artery (ACA) is one of the two terminal branches of internal carotid artery that supplies orbitofrontal and medial hemispheric portions of the brain. ACA is topographically and angiograpically divided into a precommunicating (A1) and postcommunicating (A2, also called as pericallosal artery) parts [1, 2].
Approximately 86.5% of all intracranial aneurysms arise on the anterior (carotid) circulation. Common locations include the anterior communicating artery (30%), the internal carotid artery (ICA) at the posterior communicating artery origin (25%), and the MCA bifurcation (20%). The ICA bifurcation (7.5%) and the pericallosal/calloso marginal artery bifurcation account for the remainder (4%). Distal segment of anterior cerebral artery is also one of the preferred sites for traumatic intracranial aneurysms to develop [3].
Unruptured intracranial aneurysms (UIA’s) are a major public health issue. These lesions have become increasingly recognised in recent years with advent of advanced cerebral imaging techniques. Epidemiological evidence from multiple sources suggests that intracranial aneurysms do not rupture [4]. Several autopsy studies have shown a wide range of overall frequency (0.2%-9.9%) for UIAs in the general population [5]. More recent prospective angiographic and autopsy studies indicate an overall frequency of approximately 2% to 4% in US citizens [6]. Giant aneurysm (GIA’s) are defined as aneurysm measuring more than 2.5 cm in diameter, occurrence has been reported approximately 5-13% of all intracranial aneurysms. They constitute a special group which do not usually cause sub-arachnoid haemorrhage (SAH). Instead they are commonly detected as slow growing, space occupying mass lesion. This particular aneurysm may be confused with other cerebral mass lesions, such as ingulated or pituitary adenoma. Early diagnosis is possible in this particular aneurysm using CT angiography and Magnetic resonance angiography (MRA) [7].
Case Report
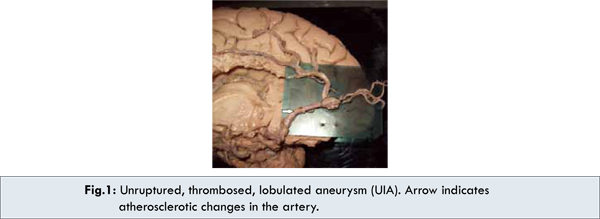
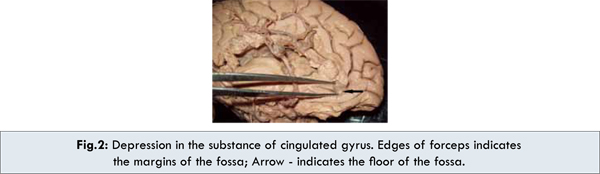
We present a case of unilateral occurrence of unruptured intracranial aneurysm (UIA) on the distal segment of anterior cerebral artery which was found during routine dissection of formalin preserved human brain. It was noted that anterior cerebral artery of the left hemisphere at about 5 cm after its origin from the left internal carotid artery, anterior to the initial part of the genu of the corpus callosum, presented a oval shaped, lobulated, thrombosed, unruptured, saccular dilatation measuring about 1.2 cm in diameter which was partially buried in the substance of cingulated gyrus producing a depression of 8 mm deep and the length of 1.5 cm antero-posteriorly [Fig.1, 2].
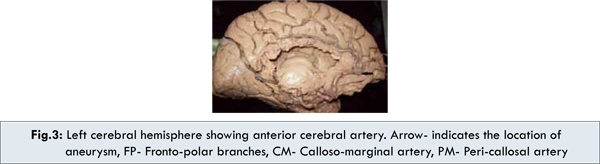
The orbital branches are given off at the initial part and fronto-polar branches arise at the location of the aneurysm itself. Later the artery curves upwards on the upper surface of the body of the corpus callosum in the callosal sulcus giving off calloso-marginal and pericallossal artery [Fig.3]. Atherosclerotic changes were also observed. No ischemic changes were observed as the brain tissue appeared normal as the opposite side suggesting that no sub- arachnoid haemorrhage has occurred. No other gross variants were observed.
Discussion
Scanty literature is available on UIA’s producing deformation of the brain tissue which in turn may cause neurological deficits. Frontal lobe dysfunction can be due to various causes like neurodegenerative, cerebro-vascular accidents, trauma, tumours and aneurysms. The risk of subarachnoid haemorrhage (SAH) is less in the case of UIA’s but these slow growing space occupying lesion can mimic like a tumour and produce clinical effects due to increased intracranial pressure and brain shift, and produces disturbed function of the particular area [8]. Frontal lobe plays a vital role in emotional pathway, memory and speech production. Brodman area number 9-12 are represented in the medial frontal gyrus which is considered as an area for abstract thinking, judgement, and decision making and also are connected to limbic system via association fibres. Cingulate gyrus contains association fibres which connect anterior nucleus of thalamus to parahippocampal area (limbic system) forming the papez circuit. Damage to this particular area can produce loss of memory and behavioural changes [9-12]. In a case report of a 67 year old patient with a large completely thrombosed giant aneurysm of anterior communicating artery (ACoA), patient had features of progressive frontal lobe psychotic syndrome for more than 12 years. CT findings showed hyperdense calcified suprasellar space occupying lesion, which was confirmed post mortem. In another case report of 31 year-old female patient suffering chronic headache was requested cranial computed tomography examination upon worsening, demonstrated the azygos anomaly of the pericallosal artery with no demonstrable aneurysm neither at the anterior communicating artery site nor distal anterior cerebral artery [13].
Glynn (1940) proposed that the most important factor in producing saccular aneurysms was degeneration of the internal elastic lamina, possibly caused by or otherwise related to atherosclerosis. He suggested that both congenital medial defects and acquired internal elastic lamina defects had to be present before cerebral aneurysms formed [14]. Locksley (1966) described 34 patients with unoperated UIAs, of whom only 19 had long-term follow-up (>5 years or until death). Among these 19 patients, 8 died of spontaneous SAH, and 1 died after lumbar puncture. All 8 patients with ruptures had aneurysms that were 7 to 11 mm in diameter or larger (precise sizes were unavailable). No aneurysm less than 7 mm in diameter ruptured, and it was not indicated whether any aneurysm less than 10 mm in diameter ruptured [15].
The 3 major modalities used to reveal and study the size, location, and morphology of an intracranial aneurysm include thin-section CT scanning after an intravenous injection using special computer software (CT angiography [CTA]; MRA and catheter angiography [16,17].
When UIAs are left untreated and monitored, it seems advisable to suggest that patients avoid smoking (and passive smoke), heavy alcohol consumption, stimulant medications and drugs, and excessive straining and valsalva manoeuvres resulting in major sudden increases in blood pressure. Daily physical activities need not be altered.
Conclusion
UIA’s are space occupying masses which can produce neurological deficits depending on their artery involved, size, and location. As in this case unruptured aneurysm (UIA) of anterior cerebral artery has produced deformation of brain tissue which would produce frontal lobe dysfunction, loss of memory and clinical effects of increased intra-cranial pressure without SAH. Therefore, it is necessary to examine for presence of UIAs in patients suffering with headache, behavioural or personality changes, speech disturbances and gait abnormalities. UIA’s should be generally monitored annually with Magnetic Resonance Angiography or CT Angiography for 2 to 3 years and then every 2 to 5 years thereafter if the UIAs are clinically and radiographically stable [18].
References
- Basar S. Monkey’s type of Anterior cerebral artery mimicking anuersym: CT angiographic findings. Neuroanatomy. 2008;5:27-29.
- Perlmutter D, Rhoton AL Jr. Microsurgical anatomy of the distal anterior cerebral artery. J Neurosurg. 1978;49:204–228.
- Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998;29:251–256.
- International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention [published correction appears in N Engl J Med. 1999;340:744]. N Engl J Med. 1998;339:1725-1733.
- McCormick WF, Acosta-Rua GJ. The size of intracranial saccular aneurysms: an autopsy study. J Neurosurg. 1970;33:422-427.
- Ronkainen A, Hernesniemi J, Puranen M, Niemitukia L, Vanninen R, Ryynanen M, et al. Familial intracranial aneurysms. Lancet. 1997;349:380–384.
- Yong-Zhong G, van Alphen HA. Pathogenesis and histopathology of saccular aneurysms: review of the literature. Neurol Res. 1990;12:249–255.
- Kenneth W Lindsay, Ian Bone. Neurology and neurosurgery illustrated. 4th edition; Churchill livingstone,2004;107-109.
- Datta AK. Essentials of Anatomy: Neuroanatomy, Volume 4, 3rd Edition, Current book international, Calcutta 2007;57-59.
- Bokemeyer C. Giant aneurysm causing frontal lobe syndrome. J Neurol.1990;237:47-50.
- Richard S Snell. Clinical Neuro-Anatomy. 6th edition; Lippincott Williams, 2001;478-479.
- Mishra PS. Variations of anterior cerebral artery in human cadavers. J Anat Soc India. 2004;35:15-16
- Baptista A. Studies on the arteries of the brain. II. The anterior cerebral artery: some anatomic features and their clinical implications. Neurology. 1963;13:825–835.
- Glynn LE. Medial defects in the circle of Willis and their relation to aneurysm formation. J Pathol Bacteriol. 1940;51:213-222.
- Locksley HB. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. J Neurosurg. 1966;25:321-368.
- Risks and benefits of screening for intracranial aneurysms in first-degree relatives of patients with sporadic subarachnoid hemorrhage. The Magnetic Resonance Angiography in Relatives of Patients with Subarachnoid Hemorrhage Study Group. N Engl J Med. 1999;341:1344–1350.
- Miyazawa N, Nukui H, Yagi S, Yamagata Z, Horikoshi T, Yagishita T, Sugita M. Statistical analysis of factors affecting the outcome of patients with ruptured distal anterior cerebral artery aneurysm. Acta Neurochir. 2000;142:1241–1246.
- Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms. Brain. 2000;123:205–221.
|
|
|
|
|
|
|
Search Google Scholar for
|
|
|
Article Statistics |
|
Joshua SA, Nayak SG, Pare VS, Ashok, Sebastian RUnruptured Intracranial Aneurysm Involving the Distal Anterior Cerebral Artery: A Cadaveric Study.JCR 2013;3:5-9 |
|
Joshua SA, Nayak SG, Pare VS, Ashok, Sebastian RUnruptured Intracranial Aneurysm Involving the Distal Anterior Cerebral Artery: A Cadaveric Study.JCR [serial online] 2013[cited 2025 Apr 26];3:5-9. Available from: http://www.casereports.in/articles/3/1/unruptured-intracranial-aneurysm.html |

|
|
|
|
|