benadryl and pregnancy cleft palate benadryl and pregnancy risks
From the Department of Paediatric Surgery and Anaesthesia1,
S.M.S. Medical College & associated SPMCHI, Jaipur-302004, India.
Corresponding Author:
Dr. Vijay Kumar Kundal
Email: vijayraksha@yahoo.com
Abstract
Teeth in newborn are called natal teeth and teeth that erupt within one month after birth are called neonatal teeth. Both present as a rare clinical entity. These teeth commonly erupt in the mandibular anterior region. The presence of these teeth may interfere with feeding and present a risk of aspiration and swallowing if they are mobile. Treatment includes extraction. Here we report a case of natal teeth, reviewed the literature regarding the etiology, clinical presentation, associated syndromes and management.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff9427020000001c01000001000400 6go6ckt5b5idvals|170 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Teeth presenting at the time of birth are called natal teeth. Teeth that erupt within one month of birth are called neonatal teeth [1]. Various terminology used for neonatal tooth includes congenital teeth, predeciduous teeth, precociously erupted teeth, premature teeth, dentition [2]. The most common site of natal and neonatal teeth is the mandibular incisor region [1,3]. Other common sites of neonatal teeth are mandibular canine region, maxillary canine and molar region [4]. The prevalence of neonatal teeth ranges from 1:700 to 1:30,000 [5].The cause of these teeth is not known but proposed hypothesis includes endocrine illness, dietary deficiencies, family history and syndromic association such as chondroectodermal dysplasia [6].
Case Report
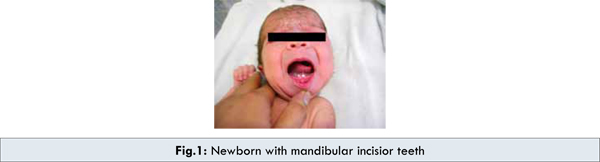
A 3 day old male child was referred to us as a case esophageal atresia with trachea-esophageal fistula (EA with TEF) with neonatal teeth in the central lower jaw [Fig.1]. Oral examination revealed two teeth in the mandibular anterior region. The teeth had whitish colouration with grade II mobility. The size of crown and appearance of gingival was normal. Rest of oral cavity was normal. Roentogram revealed natal teeth in anterior mandibular region with normally developing incisor teeth which were devoid of root. Since patient was planned for surgery for EA with TEF, both the teeth were extracted along with EA with TEF surgery. After 2 weeks, extraction sockets of both neonatal teeth were healing normally. Child was feeding normally and was comfortable.
Discussion
Primary teeth normally erupt at the age of 6 months. In rare instances, the timing of tooth eruption is significantly altered and first teeth erupt at birth or immediately after birth. Massler and Sarara have coined the terms “Natal” and “Neonatal” for teeth that erupt at birth and immediately after birth till 1 month of age respectively [1]. This terminology is based on timing of eruption and has no relation to anatomy and histology or maturity of teeth [7,8].
The incidence of natal and neonatal teeth varies from 1:1000 to 1: 30,000. Most common site of natal or neonatal teeth is mandibular incisors (85%) followed by maxillary incisors (11%), mandibular cuspids (3%) and maxillary cuspids (1%) and 1% as supernumery teeth [9]. The etiology of these teeth is unknown and are frequently found in association with developmental abnormalities and syndromes such as Ellis-Van Crevald syndrome or Hallerman-Streiff syndrome, cleft palate, Riga-Fede disease [10,11]. There is no reported association of natal or neonatal teeth with EA with TEF as in our case.
Spoug and Feasby (1966) classification is based on degree of maturity of natal and neonatal teeth [5,12]. A mature natal or neonatal tooth is fully developed with good prognosis while immature natal or neonatal tooth, refers to a tooth with incomplete or substandard structure and is associated with poor prognosis. The appearance of each natal tooth into the oral cavity can be classified into four categories as the teeth emerge into oral cavity [5,12,13]: (a) Shell-shaped crown, poorly fixed to alveolus by gingival tissue and absence of a root. (b) Solid crown, poorly fixed to the alveolus by gingival tissue and little or no root. (c) Eruption of the incisal margin of the crown through the gingival tissue. (d) Edema of gingival tissue with an un-erupted but palpable tooth. If the degree of mobility is more than 2 mm, the natal or neonatal teeth of category (a) and (b) needs extraction [2].
Clinically these natal or neonatal teeth may be of small or normal size, conical or normal shape. They may show immature appearance with enamel hypoplasia with small root. Colour varies from brown-yellowish to whitish opaque colour. They are usually attached to pad of soft tissue above alveolar ridge resulting in exaggerated mobility predisposing neonates to aspiration or swallowing.
The diagnosis of natal or neonatal teeth is based on history, oral examination and radiographic findings. Management of these teeth depends upon Spoug and Feasby(1966) classification and degree of mobility of teeth. Maintenance of mature natal and neonatal teeth is the first treatment option. If these teeth do not cause interference with breast feeding and are asymptomatic, no intervention is required. Extraction is the treatment of choice in immature natal and neonatal teeth having minimal gingival attachment, considering the risk of aspiration, Riga-Fede disease and feeding problems. Vitamin K (0.5-1.0 mg) is administered prophylactically because of risk of haemorrhage. In neonates, where there is more gingival attachment and local anaesthetic is needed for extraction, curettage of extraction site is also recommended to prevent residual teeth.
References
- Massler M, Savara BS. Natal and neonatal teeth; a review of 24 cases reported in literature. J Pediatr. 1950;36:349-359.
- Singh S, Subbareddy VV, Dhananjaya G, Patil R. Reactive fibrous hyperplasia associated with a natal tooth. A case report. J Indian Sot Pedo Prev Dent. 2004;22:183-186.
- King NM, Lee AM. Prematurely erupted teeth in newborn infants. J Pediatr. 1989;114:807-809.
- Kamboj M, Cougule R. Neonatal tooth- How dangerous can it be? J Clin Pediatr Dent. 2009;34:59-60.
- Rao RS, Mathad SV. Natal Teeth; case report and review of literature. J Maxillofac Path. 2009;13:41-46.
- Lemos LVFM, Shintome LK, Ramos CJ, Myaki SI. Natal and neonatal teeth. Einstein. 2009;7:112-113.
- Alvarez MP, Crespi PV, Shanske AL. Natal molars in Pfeiffer syndrome type 3: A case report. J Clin Pediatr Dent. 1993;18:21-24.
- Anderson RA. Natal and Neonatal teeth: Histologic investigation of two black females. ASDC J Dent Child. 1982;49:300-303.
- Anegundi RT, Sudha P, Kaveri H, Sadanand K. Natal and neonatal teeth: a report of four cases. J Indian Sot Pedo Prev Dent. 2002;20:86-92.
- Masatomi Y, Abe K, Ooshima T. Unusual multiple natal teeth, case report. Pediatr Dent. 1991;13:170-172.
- Hedge RJ. Sublingual traumatic ulceration due to neonatal teeth(Riga-Fede disease). J Indian Soc Pedod Prev Dent. 2005;23:51-52.
- Spouge JD, Feasby WH. Erupted teeth in new born. Oral Surg Oral Med Oral Pathol. 1966;22:198-208.
- Leung AKC, Robson WLM. Natal teeth: A Review. J Natl Med Assoc. 2006;98:226-228.
|