Prasad Mylarappa, Puvvada Sandeep, Prathvi, Kailash B Banale, Amey D Pathade, D. Ramesh
From the Department of Urology, MS Ramaiah Medical College and Hospital, MSRIT Post,
New BEL road, Bangalore- 560054, India.
Corresponding Author:
Dr. Prasad Mylarappa
Email: prasadmyl@rediffmail.com
Abstract
Pseudo Aneurysm of the arterial anastomosis is a rare complication seen in less than 1% of recipients and pseudo aneurysm of ileofemoral thrombosis is even rarer. Herein, we report a case of pseudo aneurysm of the anastomotic site following renal transplantation with extensive ileofemoral thrombosis with literature review. The intension of this paper is to provide an update on the varied clinical presentation, early diagnosis and management of this rare case presentation.
|
6go6ckt5b8|3000F7576AC3|Tab_Articles|Fulltext|0xf1ff74d302000000bc01000001000f00 6go6ckt5b5idvals|192 6go6ckt5b5idcol1|ID 6go6ckt5b5|2000F757Tab_Articles|Fulltext Introduction
Pseudo aneurysm of the arterial anastomosis is a rare complication seen in less than 1% of recipients and pseudo aneurysm of ileofemoral thrombosis is even rarer [1]. Due to the small series of patients and isolated case reports described in current literature, the occurrence and treatment of this potentially life threatening complication, its aetiology, indications for repair, management options and prognosis remain controversial [2]. Herein, we are reporting a case of pseudo aneurysm of the anastomotic site following renal transplantation with extensive ileofemoral thrombosis with literature review.
Case Report
58 year old patient on dialysis with end stage renal disease secondary to diabetic nephropathy underwent successful renal transplantation from a living related donor. Left kidney was harvested from the donor by the laparoscopic donor nephrectomy. After adequate renal perfusion, the renal artery graft was anastomosed to the right external iliac artery and the renal vein graft to the external iliac vein. His prophylactic immunotherapy included tacrolimus, mycophenolate mofetil and prednisolone. Allograft function was adequate in the immediate post-operative period with normalization of the renal parameters. He was discharged on tenth post operative day and advised regular follow up.
He was readmitted eight weeks after renal transplant with history of sudden onset pain and swelling in the right lower abdomen with anuria [Fig.1]. On evaluation, he was found to be anaemic with tender mass in right iliac fossa with raised serum creatinine (3.0 mg/dl). Emergency ultrasonography of abdomen and pelvis revealed heterogeneous collection around the transplanted kidney measuring 10x8x7 cm with volume of 450cc [Fig.2]. Since renal Doppler showed the normal arterial flow to the graft, he was treated conservatively with catheterization, blood transfusion and antibiotics for which he responded well with increased urine output and decreased serum creatinine. As he was planned for discharge, suddenly he had further bleeding and developed tense right lower limb swelling with increase in the size of swelling in right iliac fossa with pain.
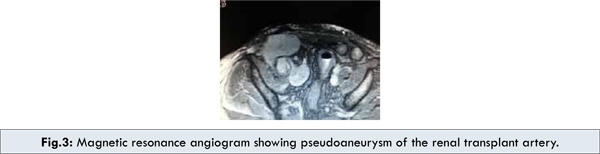
Duplex ultrasonography of the right leg and transplanted kidney demonstrated venous thrombosis of the femoral vein extending to the external iliac vein, normal arterial inflow and heterogeneous mass around the transplantated kidney. Magnetic resonance angiography done to look for source of bleeding showed the pseudo aneurysm of renal transplant artery measuring 4x3 cm at the anastomotic site compressing the external iliac vein [Fig.3]. At emergency exploration, the pseudo aneurysm was excised with graft nephrectomy and the hole in the external iliac artery was closed with saphenous vein patch. Ileofemoral thrombectomy was also done at the same sitting. Microbiological examination of the excised aneurysm wall was negative for bacteria or fungus..


Discussion
Medical or surgical complications can occur following renal transplant in up to 10% of patients [3,4]. Surgical complications usually encountered include ureteral problems (obstruction, urinoma, or lymphocele) or vascular problems (stenosis or thrombosis of renal artery, arterio venous fistula, thrombosis of renal vein or iliac vein, bleeding, perigraft hematoma or pseudo aneurysm).
The pseudo aneurysm typically occurs at the anastomotic site, extra renal [4-6] or with in the allograft [7,8]. Intrarenal pseudo aneurysms are usually secondary to acute or chronic rejections, needle biopsy of the graft kidney, whereas extra renal pseudo aneurysm have been attributed to the infection or vascular anastomotic defects [9]. When located at the anastomotic site pseudo aneurysms are commonly due to suture rupture, anastomotic leakage or vessel wall ischemia [10]. The development of pseudo aneurysm of the transplant renal artery in the anastomotic site is a rare surgical complication and occurrence of pseudo aneurysm with ileofemoral thrombosis is even rarer.
Ileofemoral thrombosis is a well recognised complication in patients undergoing major pelvic surgeries. However, the incidence of ileofemoral thrombosis after kidney transplant is uncertain, varying from 0.8 to 25% [11]. The ileo-femoral thrombosis in pseudo aneurysm of graft is very rare. Possible reasons include a pelvic dissection, venous anastomosis with clamping of the vein, decreased venous emptying secondary to the position of the kidney, mechanical compression by hematoma or pseudo aneurysm or lymphocele [11]. Other well defined risk factors include age more than 40 years, obesity, history of venous thromboembolism, bed rest more than 5 days [11]. Only clinical features of pain, swelling and calf tenderness cannot be used to diagnose deep vein thrombosis, but these clinical features alert one to obtain further testing to know the underlying diagnosis. In rare occasion, as in our case, presumably ileofemoral thrombosis occurred due to compression of external iliac vein by pseudo aneurysm of the graft renal artery and the perigraft hematoma. Duplex ultrasonography has now replaced the venography as the most widely used diagnostic test for the deep vein thrombosis with excellent sensitivity and specificity of 97% and 94% respectively [11]. Computerised Tomographic Angiography/ Magnetic Resonance Angiography are widely used to diagnose pseudo aneurysm of transplant renal artery.
Therapeutic options include anticoagulants to prevent clot extension, graft loss and pulmonary embolism. The current options are unfractionated heparin, low molecular weight heparin and warfarin. Venous thrombectomy is considered for the ileofemoral thrombosis following renal transplantation. Early clot removal is achieved by either mechanical thrombectomy using an open or endo vascular approach or catheter directed thrombolysis. In our case, since ileofemoral thrombosis was associated with the bleeding pseudo aneurysm of renal artery, emergency exploration with graft nephrectomy with venous thrombectomy was done. The rent in external iliac artery was closed with saphenous vein patch.
Conclusion
The development of pseudo-aneurysm of the anastomotic site with extensive ileo-femoral thrombosis following renal transplant is a rare complication and only few isolated cases have been reported in literature. Due to serious complication that can arise from large pseudo-aneurysm as in our case, we feel increased clinical awareness and close monitoring in the post operative period is required. The benefits derived from early diagnosis and treatment is indispensable.
References
- Koo CK, Rodger S, Baxter GM. Extra-renal pseudoaneurysm: an uncommon complication following renal transplantation. Clin Radiol. 1999;54:755-758.
- Bracale UM, Carbone F, del Guerico L, viola D, D’Armiento FP, Maurea S, Porcellini M, Giancarlo Bracale. External iliac artery pseudoaneurysm complicating renal transplantation. Interactive cardiovascular and thoracic surgery. 2009;8:654-660.
- Matas AJ, Payne WD, Sutherland DER, Humar A, Gruessner RW. 2,500 loving donor kidney transplants: a single-center experience. Ann Surg. 2001;234:149-164.
- Gerbens D, Teyssou H, Manteau G, Ruiz R, Bureau M, Tessier JP. Ultrasonography and surgical complications after kidney transplants. J Radiol. 1980; 61:405-410.
- Yap R, B Madrazo, Oh HK, Dienst SG. Perirenal fluid collection after renal transplant. Am Surg. 1981;47:287-290.
- Streeter EH, Little DM, Cranston DW, Morris PJ. The urological complications of renal transplantation: a series of 1535 patients. BJU Int. 2002;90:627-634.
- Grenier N, Douws C, Morel D, Ferriere JM, Le Guillou M, Potaux L, Broussin J et al. Detection of vascular complications in renal allografts with color Doppler flow imaging. Radiology 1991;178:217-223.
- Koo CK, Rodger S, Baxter GM. Extra-renal Pseudoaneurysm: an uncommon complication following renal transplantation. Clin Radiol. 1999;54:755-758.
- Luzzio CC, Waclawik AJ, Gallarcher CL, Knechtle SJ. Iliac artery pseudoaneurysm following renal Transplantation presenting as lumbosacral plexopathy. Transplantation 1999;67:1077-1078.
- Baxter GM: Ultrasound of renal transplantation. Clin Radiol. 2001;56:802-818.
- Gang S, Rajapurkar M. Vascular complications following renal Transplantation. Journal of Nephrology and Renal Transplantation. 2009;2:122-132.
|